Transparency Grade: F
Overall Performance FY2024-2025
What's the data showing?
Obtained via FOI, this shows a breakdown of costs, recruitment and visits for BC's UPCCs. These health authority operated clinics were originally supposed to provide ongoing primary care (i.e., attachment), episodic primary care for unattached patients, and urgent care (to reduce ER visits), all using a team-based care model.
Promises were made that information on UPCC performance would be regularly reported to the public, but this hasn't happened.
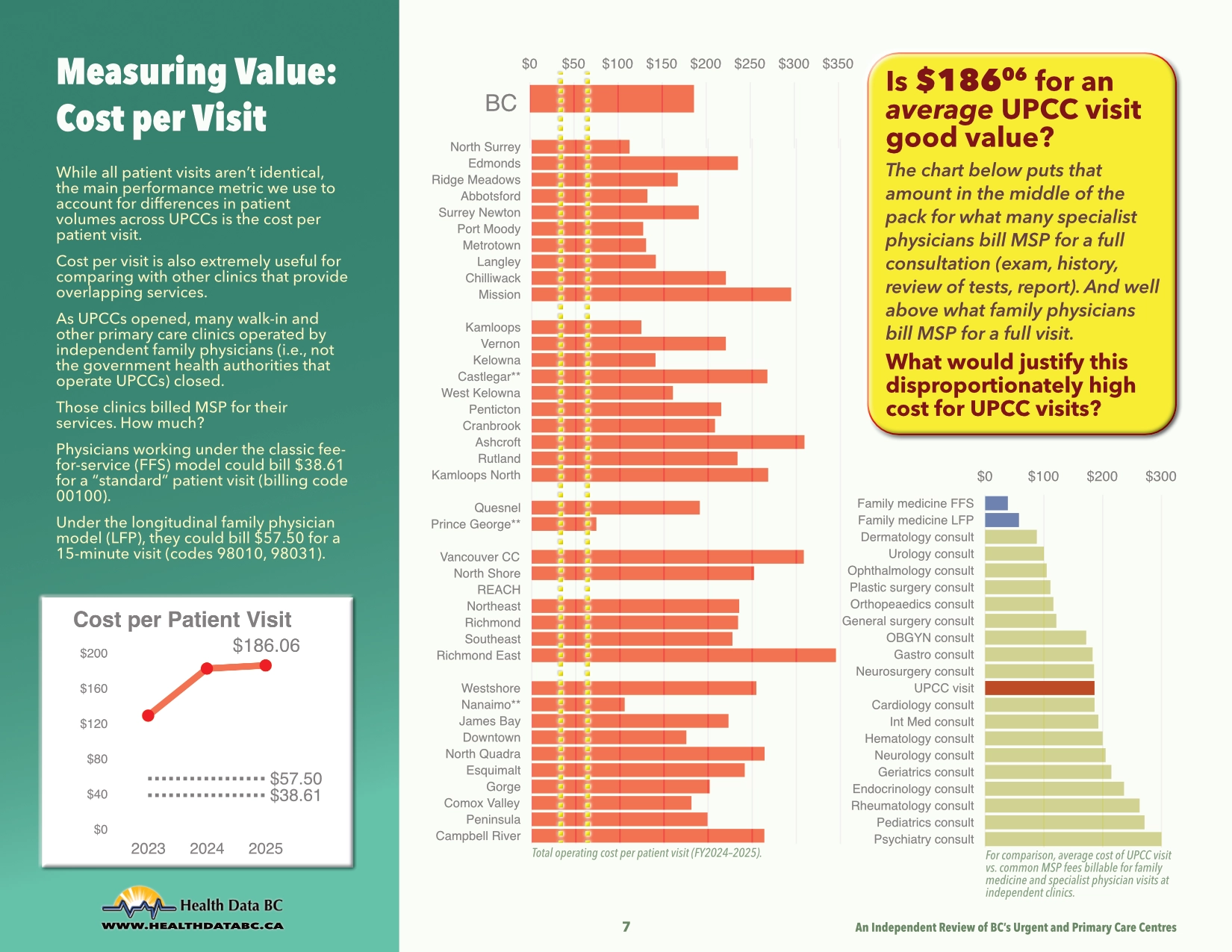
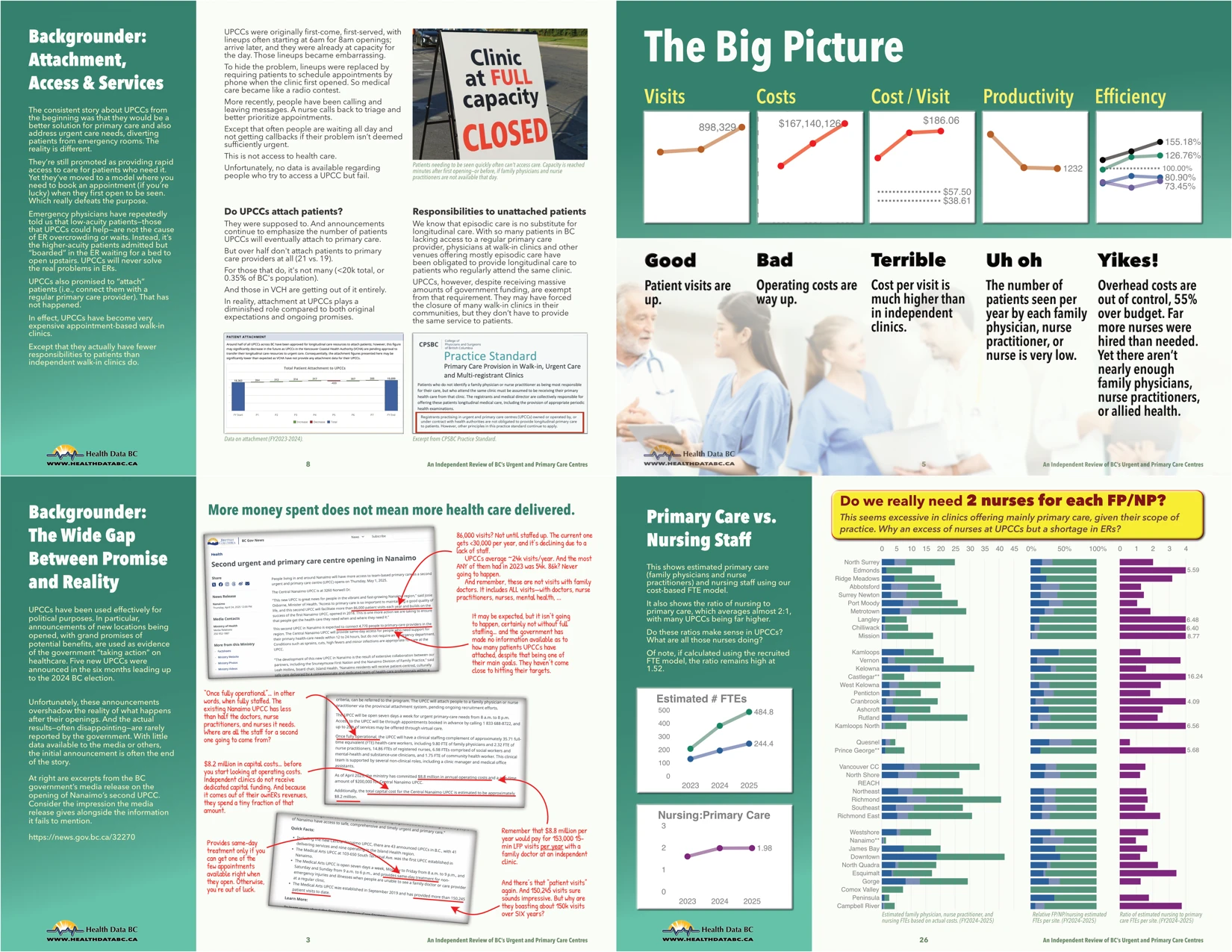
- average cost per visit $186.06
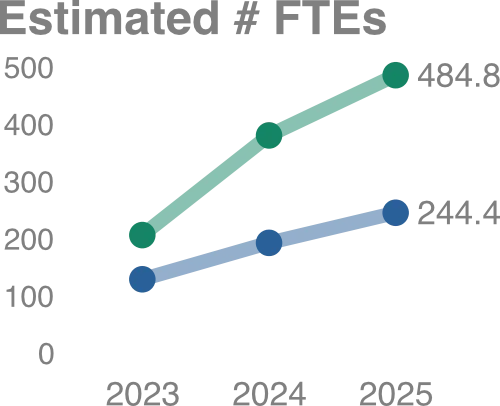
- 16-27% understaffed on family physicians, nurse practitioners, allied health
- 27% overstaffed on nurses (who are likely needed far more elsewhere)
- 2:1 nursing:primary care ratio
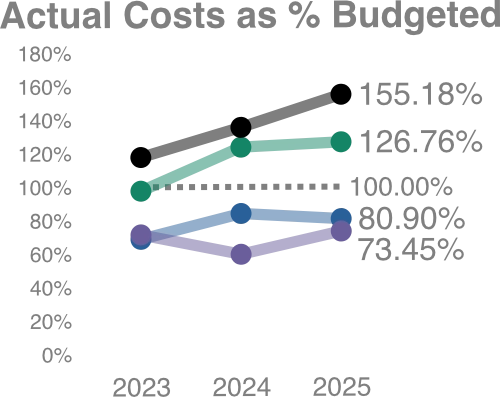
- 55% over budget on overhead
- limited patient attachment
- limited access for urgent care
- very low patient volumes given resources
- excessive performance differences across sites
- administrator-heavy, with limited accountability for results or expenditures
 UPCCs have twice the nursing staff vs. primary care (FP/NP).
Why so many in a primary care setting? What are they all doing?
UPCCs have twice the nursing staff vs. primary care (FP/NP).
Why so many in a primary care setting? What are they all doing?
They can't diagnose, order tests, refer to specialists, prescribe meds…
Yet, ERs close for lack of nurses.
 UPCC financials tell a worrying tale:
UPCC financials tell a worrying tale:
- many can't recruit/retain core staff (20% short of FPs, 16% NPs), allied health (27%)
- 27% OVER-spending on nurses
- excessive overhead (>31% of costs); an insane 55% over budget (11 sites spend double their budget)
Download the Full Report
🟢 Download upcc2025.pdf
[PDF, 30 pages, 8.7MB, last updated Jun 8/2026]
Analysis of data obtained via freedom of information requests (2022-2025).
What's the opportunity?
A lot of money and resources have been devoted to UPCCs, often at the expense of independent primary care clinics. UPCCs have not met their goals, are inefficient, have high overhead (greatly exceeding budgets), provide limited care, and are far more costly. Lack of public scrutiny has enabled this poor use of resources.
There have been significant concerns about management and clinical policies, as well as the "divide and conquer" model of team-based care they offer. This is reflected in the difficulty staffing them with primary care providers (physicians and nurse practitioners).
Overhauling them or (better) turning their operation over to management with familiarity operating primary care clinics (vs. large hospitals) would make far better use of the resources.
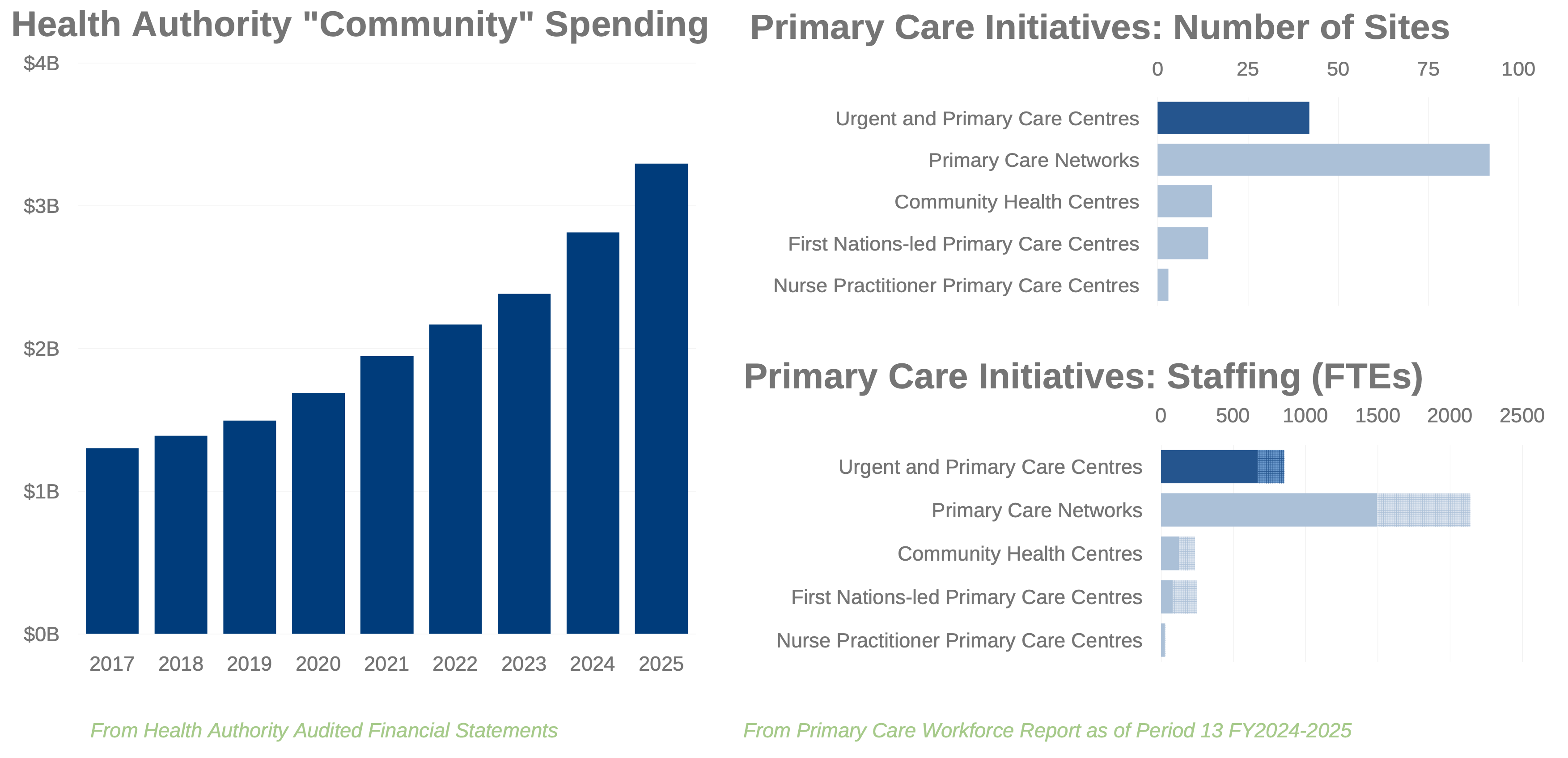
UPCCs are just the start of health authority incursion into primary care. Spending on "community" is up 2.5x since NDP took power, second only to "corporate" increases. We know little about the performance of other primary care initiatives they're involved with. What would we find if the entire $3.3 billion (and 2400+ FTE staff, with another 1000+ FTE approved) underwent the same scrutiny as the $167 million for UPCCs described here?
Sources
FOI Requests
UPCC FY2024-2025 cost/visit/staffing data
UPCC FY2023-2024 cost data [source]
UPCC FY2023-2024 visit/staffing data [source]
UPCC FY2022-2023 cost data [source]
UPCC FY2022-2023 visit/staffing data [source]
FOI data in Excel
Includes raw data incorporated from above FOI requests, derived values, and all charts from the report.
What's missing?
There's no public access to this information; it required a FOI request that took five months (and $430) for the most recent year (the previous year took twice as long).
We still need much more information on what clinical services staff are providing to explain the extremely high cost per visit. As well as times when needed clinical staff (i.e., FPs/NPs) are not available.
There is no information available on access, in particular how difficult it is for people to get seen at a UPCC; the "radio contest" call-in-at-8am model is a significant barrier.